You may take levothyroxine for years. Maybe for life. That makes a very reasonable question hard to ignore: if this is going to be part of your routine long term, how safe is it really?
Here is the short answer: levothyroxine is generally safe long term when it is replacing a hormone your body actually needs and the dose is monitored over time. The biggest long-term problems usually do not come from the existence of thyroid hormone replacement itself. They come from staying on the wrong dose for too long, especially a dose that is too high.
That distinction matters. According to FDA and DailyMed labeling, chronic over-replacement can increase cardiac strain and lower bone mineral density, particularly in older adults and postmenopausal women. The American Thyroid Association makes the same basic point in plainer language: too much thyroid hormone raises the risk of heart rhythm problems and bone loss. In other words, the long-term safety question is usually a dose-management question, not a “this drug is toxic” question.
In this guide, you will learn when long-term levothyroxine use is considered safe, what the real long-term risks are, which patients need closer follow-up, and what practical habits keep long-term treatment safer.
The Quick Answer
For most people who truly need thyroid hormone replacement, levothyroxine is safe to take long term.
What makes long-term treatment safe:
- the diagnosis is correct
- the dose is appropriate
- TSH and symptoms are reviewed over time
- interactions and absorption problems are addressed
- life changes such as aging, pregnancy, weight change, or brand switching trigger re-checks
What makes long-term treatment less safe:
- chronic over-treatment
- chronic under-treatment
- assuming the original dose is always the right dose
- taking it inconsistently or too close to interfering supplements and medications

Long-term safety depends on follow-up, not just the prescription itself
For most patients, levothyroxine stays safe over time when the dose is reviewed against symptoms, lab trends, and life changes rather than left on autopilot for years.
What “Long-Term Safety” Really Means
When patients ask whether levothyroxine is safe long term, they are usually asking one of four things:
- Will this hurt my heart?
- Will this weaken my bones?
- Will my body become dependent on it in a harmful way?
- If I take it for years, could I slowly end up on the wrong dose without realizing it?
Those are not all the same question.
Levothyroxine is synthetic T4, a version of the same hormone your thyroid naturally makes. When your body is not producing enough thyroid hormone, replacement is physiologic. The goal is not to “stimulate” your thyroid or force an unnatural state. The goal is to restore a normal one.
That is why many people do very well on levothyroxine for decades. The medication itself is not usually the long-term problem. The risk appears when the replacement level drifts too high, too low, or too inconsistent for the person taking it.
| Long-term question | What it usually means | What to review |
|---|---|---|
| “Is this safe to take for life?” | Is replacement itself harmful? | Whether you have a permanent reason to need it |
| “Can this hurt my heart?” | Possible over-treatment | TSH, pulse, palpitations, cardiac history |
| “Can this cause osteoporosis?” | Possible chronic over-replacement | Age, menopausal status, fracture risk, TSH trend |
| “Why do I still feel bad after years on it?” | Dose, absorption, diagnosis, or another cause | Labs, timing, interactions, symptoms, coexisting conditions |
Why Levothyroxine Itself Is Usually Not the Problem
For patients with Hashimoto’s disease, thyroidectomy, radioactive iodine treatment, congenital hypothyroidism, or other persistent hypothyroid states, levothyroxine is replacing something the body cannot make adequately on its own.
That is very different from taking a medication that introduces an entirely foreign physiologic effect. In most patients, well-dosed levothyroxine supports normal metabolism, normal organ function, and symptom control. The ATA’s thyroid hormone treatment guidance treats it as standard replacement therapy for precisely that reason.
The more useful question is not, “Is taking T4 for years inherently dangerous?” The more useful question is, “What happens if I am over-replaced, under-replaced, or poorly monitored for years?”
That is where the real long-term safety discussion begins.
The Main Long-Term Risks Come From Too Much Thyroid Hormone
FDA and DailyMed labeling consistently frame most levothyroxine adverse effects as manifestations of overdosage or excessive replacement. Over time, that matters most in two places: the heart and the skeleton.
Heart Rhythm and Cardiovascular Strain
If levothyroxine pushes the body toward hyperthyroidism, the heart is one of the first organs to notice. A dose that is too high can raise heart rate, increase the workload on the heart, and make rhythm problems more likely.
The concerns are not just theoretical. Both official labeling and ATA patient guidance warn about palpitations and rhythm complications when thyroid hormone is excessive. Older adults are especially vulnerable because they have less physiologic reserve and are more likely to have underlying cardiovascular disease.
Long-term warning signs that deserve review include:
- new or worsening palpitations
- resting fast pulse
- shakiness or tremor
- feeling unusually wired or anxious
- heat intolerance
- new insomnia
- unexplained weight loss
If that pattern sounds familiar, Heart Palpitations and Levothyroxine and Dose Adjustment and TSH Monitoring are the two most useful related reads.
Bone Loss and Fracture Risk
The other major long-term concern is bone health. Official labeling warns that over-replacement may decrease bone mineral density, especially in postmenopausal women. The mechanism is straightforward: too much thyroid hormone accelerates bone turnover. Over time, that can weaken bone.
A widely cited BMJ study in older adults also linked current levothyroxine use, especially at higher cumulative exposure, with increased fracture risk. That does not mean levothyroxine is unsafe for older adults. It means older adults have less margin for chronic overtreatment.
This is why long-term safety is not just about whether you take levothyroxine. It is about whether you stay slightly over-replaced for years without anyone noticing.
Who Is Most Sensitive to Over-Treatment?
- older adults
- postmenopausal women
- people with osteoporosis or high fracture risk
- patients with atrial fibrillation or other rhythm history
- patients taking suppressive doses after some thyroid cancers
These patients can still take levothyroxine safely. They simply need tighter follow-up and less casual dosing drift.
Under-Treatment Also Has Long-Term Costs
It is easy to focus so much on over-treatment that the other half of the equation gets ignored.
If your dose stays too low for months or years, the main issue is not classic drug toxicity. The issue is that hypothyroidism remains inadequately treated. According to ATA and NIDDK patient guidance, persistent hypothyroid states can leave patients with fatigue, constipation, cold intolerance, dry skin, cognitive slowing, menstrual disruption, and adverse lipid effects.
In real life, under-treatment causes two kinds of long-term problems:
Ongoing Symptom Burden
You may continue to feel like your body is running in low-power mode:
- fatigue
- slower thinking or brain fog
- constipation
- low mood
- dry skin and hair changes
- reduced exercise tolerance
Metabolic and Cardiovascular Consequences
Untreated or undertreated hypothyroidism can contribute to unfavorable cholesterol patterns and broader cardiometabolic strain. So while overtreatment gets most of the “side effect” attention, undertreatment is not benign just because it feels quieter.
This is one reason the question “is levothyroxine safe long term?” can be misleading. For many patients, the alternative to treatment is not “no risk.” The alternative is ongoing hypothyroidism.
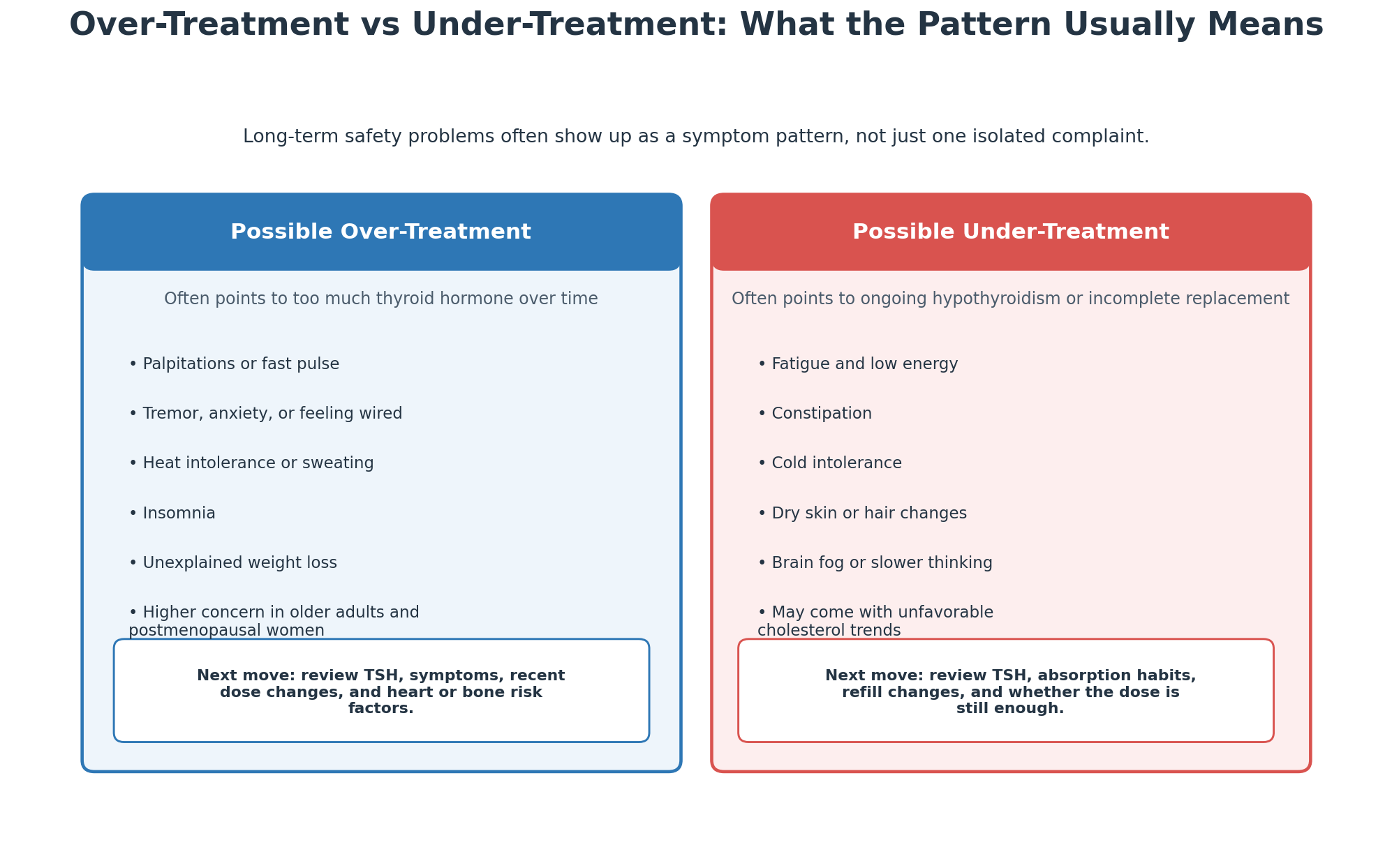
A symptom pattern often tells you more than a single complaint
Palpitations, tremor, insomnia, and weight loss point in a different direction than fatigue, constipation, cold intolerance, and brain fog. The pattern matters when you decide whether the next step is a dose review, an absorption review, or broader follow-up.
Who Needs Extra Attention Over Time?
Long-term levothyroxine treatment is not one-size-fits-all. The same tablet can be low risk in one patient and require close surveillance in another.
Older Adults
Older patients are more likely to experience palpitations, atrial fibrillation, weight loss, and fracture-related consequences from a dose that is a little too high. Endotext reviews on hypothyroidism in older adults repeatedly emphasize starting lower and titrating carefully for that reason.
Postmenopausal Women
This group has less protection against bone loss to begin with. If thyroid hormone replacement drifts too high, the cumulative effect on bone health matters more.
Patients With Heart Disease
People with coronary disease, heart failure, or prior rhythm problems need thoughtful dosing because sudden or chronic excess thyroid hormone increases myocardial demand.
Pregnancy
Pregnancy is different because thyroid hormone requirements often rise. What looks like “overtreatment risk” in one life stage can become “undertreatment risk” in another. If pregnancy is relevant, Pregnancy Dosing Adjustments matters more than generic long-term advice.
Patients With Absorption Problems
Long-term safety also depends on getting a stable amount of medication into the bloodstream. Celiac disease, inflammatory bowel disease, bariatric surgery, atrophic gastritis, and interacting supplements can all make a perfectly reasonable dose behave unpredictably.
That is why long-term safety depends partly on habits:
- taking the medication consistently
- keeping calcium and iron separated
- reviewing new medications
- being careful after brand or manufacturer changes
If your pharmacy changed products recently, Switching Between Brands and Generics is relevant.

Long-term safety also depends on daily habits at home
A stable long-term dose only works if the medication is taken consistently and common absorption problems such as calcium, iron, and refill changes are managed before they start pushing TSH off course.
How Monitoring Keeps Long-Term Use Safe
The safest long-term levothyroxine strategy is not “set the dose once and forget it.” It is steady monitoring with sane triggers for re-checking.
Typical Monitoring Rhythm
| Situation | Common follow-up |
|---|---|
| New start or dose change | Recheck TSH in about 6-8 weeks |
| Stable long-term therapy | Periodic TSH review, often every 6-12 months |
| Pregnancy | More frequent monitoring, especially early |
| Brand/manufacturer switch | Recheck if symptoms change or clinician advises |
| Major weight change, aging, new interacting medication | Consider earlier repeat labs |
The exact interval depends on the patient, but the principle is consistent: long-term safety depends on not letting dose drift go unchecked.
What Good Long-Term Monitoring Looks Like
- labs are interpreted with symptoms, not in isolation
- timing and absorption habits are reviewed
- major life changes trigger a re-check
- the same symptoms are not blamed on “just aging” without reviewing thyroid status
Some patients assume long-term safety means “I have been on this for years, so I must be fine.” That is not how replacement therapy works. What keeps it safe is ongoing calibration.
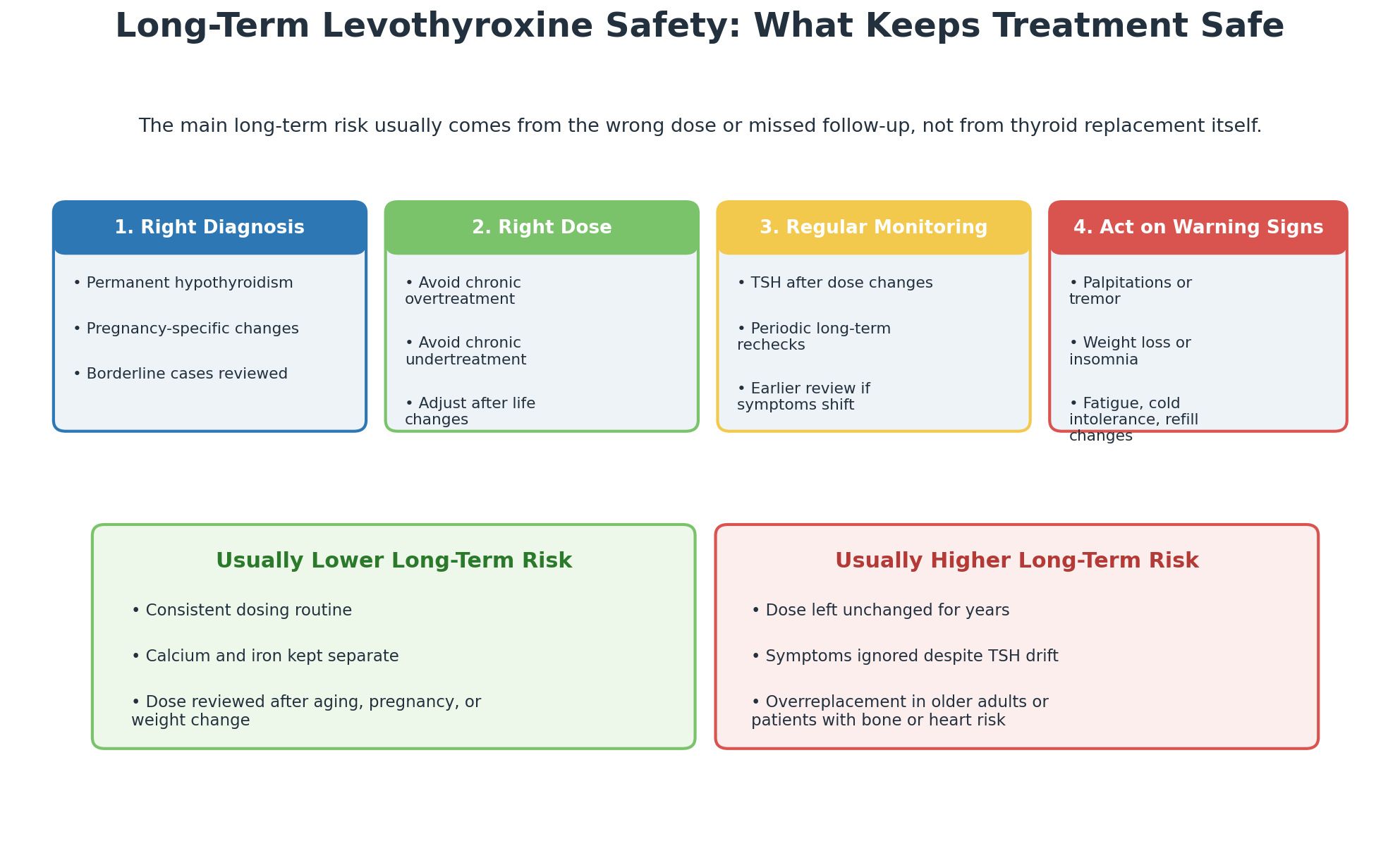
The four checkpoints that keep long-term levothyroxine use safe
The safest long-term pattern is simple: confirm the diagnosis, keep the dose appropriate, recheck TSH when circumstances change, and act early when symptoms suggest drift toward over- or under-treatment.
Signs Your Long-Term Safety Plan Needs a Recheck
Call for a routine follow-up rather than waiting for your next annual visit if you notice:
- new palpitations
- unexplained weight loss
- worsening insomnia
- new tremor or feeling overstimulated
- ongoing fatigue despite good adherence
- constipation, cold intolerance, or dry skin returning
- a major shift after a pharmacy refill change
- calcium, iron, antacid, or supplement use drifting closer to your dose
One practical rule helps: if your symptoms changed, your refill changed, or your life stage changed, your thyroid plan may need to change too.
For a broader symptom overview, Complete List of Levothyroxine Side Effects is the companion piece.
Does Levothyroxine Cause Dependency or Damage the Thyroid?
This is one of the most common fears, and it helps to separate emotional truth from physiologic truth.
If you need levothyroxine because your thyroid is permanently under-functioning, taking replacement does not “create” dependency in the usual medication sense. The ongoing need is mainly created by the underlying disease, not by the tablet.
Examples:
- after thyroidectomy, the body no longer has normal thyroid tissue to produce hormone
- with Hashimoto’s, the gland may not reliably make enough hormone
- after radioactive iodine, production may be permanently reduced
In those cases, the need for long-term treatment reflects the thyroid problem itself.
There are exceptions. Some people are placed on levothyroxine after transient thyroiditis, postpartum thyroid inflammation, or borderline situations that later resolve. In those cases, long-term treatment may not always be necessary forever. But that is a diagnosis and follow-up question, not a reason to stop medication on your own.
Do You Always Need Levothyroxine for Life?
Not always, but often.
You are more likely to need lifelong therapy if you have:
- Hashimoto’s with established hypothyroidism
- thyroid removal
- radioactive iodine treatment
- congenital hypothyroidism
- central hypothyroidism requiring replacement
You may not always need permanent therapy if the original problem was temporary or borderline, such as:
- some cases of postpartum thyroiditis
- some transient thyroiditis episodes
- some mild or uncertain subclinical hypothyroid cases
That last point matters because long-term safety includes diagnostic accuracy. If the original indication was weak, reassessment may be appropriate. But any trial off therapy should be clinician-guided, with a plan for repeat labs.
When to Get Help Right Away
Long-term safety problems usually build gradually, but some symptoms deserve urgent attention.
Seek prompt medical care if levothyroxine use is paired with:
- chest pain
- fainting
- severe shortness of breath
- a new sustained rapid heartbeat
- severe confusion
- signs of an allergic reaction such as facial swelling, hives, or wheezing
These are not routine “dose tweak” symptoms.
Frequently Asked Questions
Is levothyroxine safe long term?
Yes, for most patients who truly need thyroid hormone replacement. Long-term safety is generally good when the dose is appropriate, monitoring continues, and absorption issues are addressed.
What are the real long-term risks of levothyroxine?
The main long-term risks come from chronic over-treatment or under-treatment. Over-treatment raises concern for heart rhythm problems and bone loss. Under-treatment leaves hypothyroid symptoms and metabolic consequences in place.
Can levothyroxine cause osteoporosis?
Correctly dosed replacement is not the same thing as causing osteoporosis. The concern is chronic overtreatment, especially in postmenopausal women and older adults, where excessive thyroid hormone can accelerate bone loss.
Can levothyroxine damage the heart?
The wrong dose can stress the heart. A dose that is too high can contribute to palpitations, fast heart rate, and rhythm problems, especially in patients who are older or already have cardiac disease.
Does taking levothyroxine for years make your body dependent on it?
Usually no in the harmful sense. If you need long-term replacement, that is generally because your thyroid condition is persistent, not because levothyroxine created a new dependency.
How do I make long-term levothyroxine use safer?
Take it consistently, separate it from interfering supplements, keep follow-up lab appointments, and request a review after pregnancy, major weight change, refill changes, or new symptoms.
Key Takeaways
- Levothyroxine is usually safe long term when it is replacing hormone your body needs and the dose stays appropriate.
- The biggest long-term risks come from over-treatment, especially heart rhythm problems and bone loss.
- Under-treatment also matters because persistent hypothyroidism carries symptom and metabolic costs of its own.
- Older adults, postmenopausal women, and patients with heart disease need closer long-term dose review.
- Long-term safety depends on monitoring, consistency, and interaction management more than on fear of the medication itself.
- If your symptoms, refill, or life stage changed, it is time to review the plan rather than assume the old dose is still right.
For most patients, levothyroxine is not dangerous because it is taken for years. It becomes risky when long-term treatment turns into long-term autopilot. The safest approach is to treat it like what it is: a useful replacement therapy that needs periodic recalibration as your body and circumstances change.
Sources
- FDA. Levothyroxine Sodium Tablets prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/021116s027lbl.pdf
- DailyMed. LEVOXYL (levothyroxine sodium tablets) label. https://www.dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=951c6e16-7251-42ed-ac19-d8367a6aee4f&type=display
- American Thyroid Association. Thyroid Hormone Treatment FAQ. https://www.thyroid.org/wp-content/uploads/patients/brochures/ata-hormone-treatment-faq.pdf
- American Thyroid Association. Hypothyroidism brochure. https://www.thyroid.org/wp-content/uploads/patients/brochures/Hypothyroidism_web_booklet.pdf
- NIDDK. Hypothyroidism (Underactive Thyroid). https://www.niddk.nih.gov/health-information/endocrine-diseases/hypothyroidism
- Turner MR, et al. Levothyroxine dose and risk of fractures in older adults. BMJ. https://pubmed.ncbi.nlm.nih.gov/21527461/
- Endotext. Hypothyroidism in Older Adults. https://www.ncbi.nlm.nih.gov/books/NBK279005/